Back pain stems from multiple causes, with muscle strain leading the list, followed by disc problems, arthritis, and postural issues. The causes of back pain range from sudden injury to gradual degeneration, but most cases respond well to conservative treatments like physical therapy, lifestyle changes, and targeted exercises. Relief strategies in 2026 emphasize non-surgical approaches, combining movement therapy with anti-inflammatory lifestyle modifications and, when appropriate, minimally invasive procedures.
Key Takeaways
Muscle strain and sprain account for the majority of acute back pain cases, typically resolving within weeks with proper rest and movement
Disc-related problems (herniation, bulging, degeneration) cause pain through nerve compression and require targeted treatment from physical therapy to advanced procedures
Arthritis and joint degeneration develop gradually with age, causing chronic stiffness and aching that responds to anti-inflammatory strategies
Postural dysfunction from prolonged sitting creates persistent lower back stress, especially in desk workers and sedentary individuals
Biopsychosocial factors including stress, sleep quality, and nutrition significantly influence pain severity and recovery speed
Core strengthening (not traditional crunches) provides the most effective long-term protection against recurrent episodes
Inversion therapy offers drug-free spinal decompression that relieves pressure on compressed discs and nerves
Anti-inflammatory lifestyle changes including hydration, omega-3 intake, and weight management reduce chronic pain triggers
Early intervention prevents acute pain from becoming chronic disability
Most back pain improves without surgery when patients follow evidence-based conservative treatment protocols
What Are the Most Common Causes of Back Pain?
Muscle strain or sprain causes the majority of back pain episodes. This injury occurs when muscle fibers or ligaments tear from overuse, improper lifting technique, sudden movements, or repetitive stress. The damaged tissue triggers localized pain, tightness, muscle spasms, and limited flexibility in the affected area.
Primary muscle strain triggers include:
Lifting heavy objects with bent back instead of bent knees
Twisting the spine while carrying weight
Sudden jerking movements during sports or physical activity
Repetitive motions that fatigue muscles over time
Maintaining awkward positions for extended periods
Weak core muscles that fail to support the spine properly
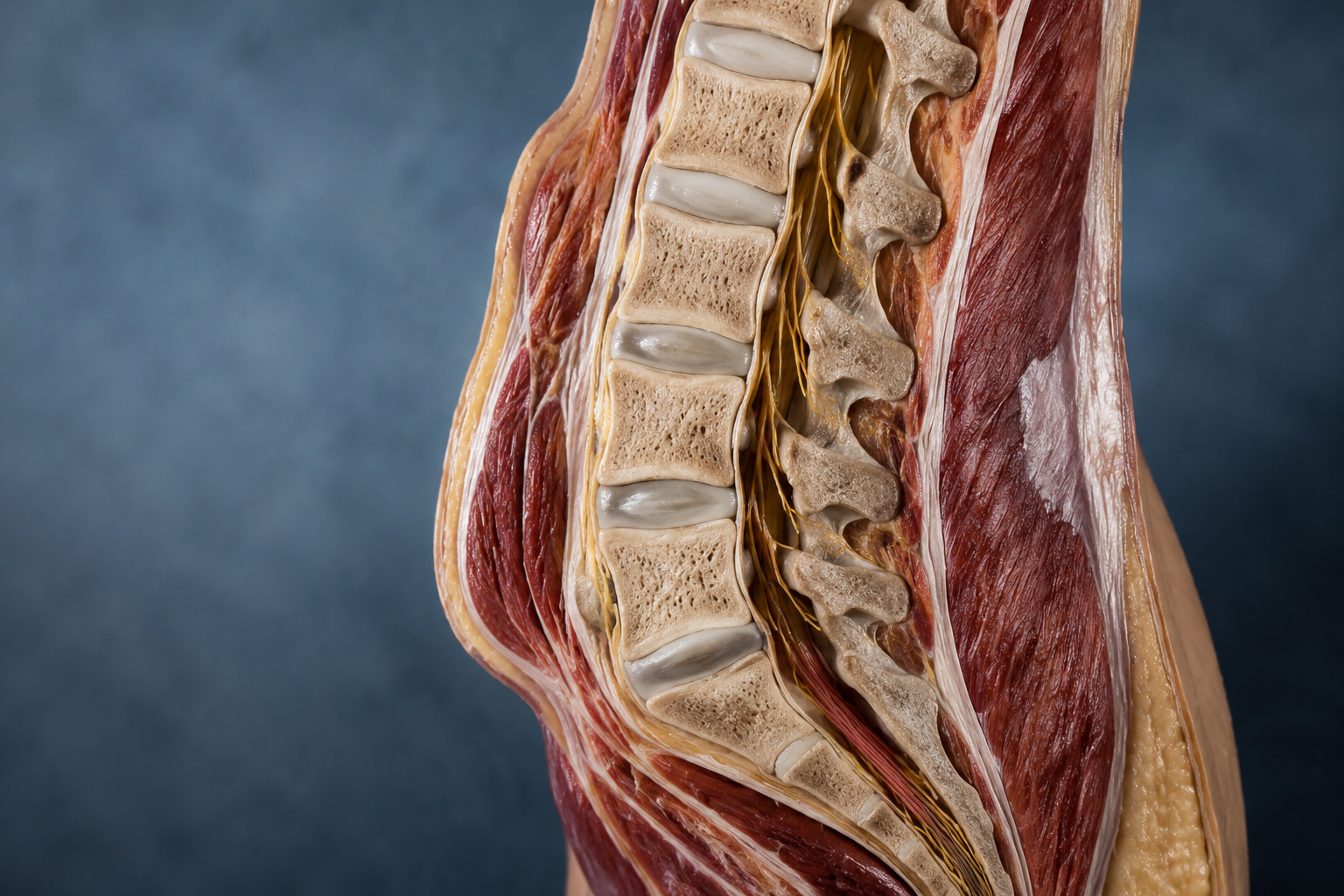
Disc-related problems rank as the second most common cause. Herniated or bulging discs develop when the soft inner material of an intervertebral disc protrudes through its outer layer, pressing on nearby nerves. This compression creates sharp, radiating pain that often travels down the leg (sciatica). Disc issues arise from acute injury, repetitive stress, or age-related degeneration.
Degenerative disc disease accelerates with age as spinal discs lose water content and cushioning ability. The condition worsens with activities that compress the spine—sitting, bending forward, and lifting. Patients experience chronic aching that intensifies during these movements and improves with position changes.
Osteoarthritis breaks down cartilage in the facet joints that connect vertebrae. This wear-and-tear condition produces morning stiffness, persistent aching, reduced range of motion, and pain that worsens with activity. The inflammation can narrow the spinal canal, creating additional nerve pressure.
Choose professional evaluation if: pain persists beyond 4-6 weeks, radiates down legs, accompanies numbness or weakness, or follows significant trauma. These red flags suggest structural problems requiring imaging and specialist care.
How Does Poor Posture Contribute to Back Pain?
Poor posture creates sustained mechanical stress on spinal structures. When you slouch at a desk or crane your neck forward to view screens, your spine moves out of its natural alignment. This misalignment forces muscles to work harder to maintain position, leading to fatigue, tension, and eventual pain.
The sitting epidemic affects millions of office workers and remote employees. Prolonged sitting increases disc pressure by 40% compared to standing. The forward-leaning position common during computer work compounds this stress, stretching posterior ligaments and compressing anterior disc material. Over months and years, this repetitive strain degrades disc integrity and weakens supporting muscles.
Postural dysfunction manifests as:
Central lower back stiffness after sitting sessions
Pain that improves with standing and movement
Gradual onset rather than sudden injury
Bilateral (both sides) discomfort rather than one-sided
Tightness in hip flexors and hamstrings
Rounded shoulders and forward head position
Asymmetrical habits create one-sided problems. Carrying bags on the same shoulder, favoring one leg while standing, or twisting repeatedly in one direction during work tasks produces uneven muscle development. The stronger side compensates for the weaker side, creating imbalances that manifest as right-side or left-side lower back pain.
Hip mobility limitations force the lower back to compensate during movement. When hips lack adequate flexion and rotation range, the lumbar spine moves excessively to complete tasks like bending or reaching. This compensation pattern overloads lumbar joints and discs, accelerating wear and triggering pain episodes.
Correction requires: ergonomic workspace setup with monitor at eye level, chair supporting lumbar curve, feet flat on floor, and regular movement breaks every 30-45 minutes. Targeted stretching for hip flexors and hamstrings, combined with core strengthening, restores proper movement patterns.
What Role Do Herniated Discs Play in Causing Back Pain?
Herniated discs compress nerve roots exiting the spinal column. The disc’s gel-like nucleus pulposus pushes through tears in the tough outer annulus fibrosus, creating a bulge that impinges on adjacent neural tissue. This mechanical pressure triggers sharp, electric pain that follows the nerve’s path—often shooting down the buttock and leg.
Herniation mechanisms include:
Acute trauma from falls, accidents, or heavy lifting
Cumulative microtrauma from repetitive bending and twisting
Age-related disc degeneration that weakens outer layers
Genetic predisposition to weaker disc structure
Smoking, which reduces disc nutrition and healing capacity
Symptom patterns help identify disc problems. Patients report pain that worsens with sitting, forward bending, coughing, or sneezing—activities that increase disc pressure. Pain improves with standing, walking, or lying down. Numbness, tingling, or weakness in specific leg muscles indicates which nerve root suffers compression.
The L4-L5 and L5-S1 discs (lowest two lumbar levels) herniate most frequently due to their position at the spine’s pivot point. L4-L5 herniation affects the L5 nerve root, causing pain down the outer leg to the top of the foot. L5-S1 herniation compresses the S1 nerve, producing pain down the back of the leg to the heel.
Conservative treatment succeeds in 80-90% of herniated disc cases within 6-12 weeks. The body resorbs herniated material through inflammatory processes, reducing nerve pressure naturally. Physical therapy emphasizes extension exercises that shift disc material away from nerves, core strengthening to reduce spinal load, and nerve gliding techniques to improve mobility.
Minimally invasive options address persistent cases. Epidural steroid injections deliver anti-inflammatory medication directly to the affected nerve root, providing weeks to months of relief. Radiofrequency ablation uses heat to disable pain-transmitting nerve fibers. Microdiscectomy surgically removes herniated material when conservative care fails after 6-12 weeks or when progressive neurological deficits develop.
Avoid: prolonged bed rest (worsens outcomes), excessive forward bending during acute phase, and premature return to heavy lifting before core strength rebuilds.
How Does Degenerative Disc Disease Develop Over Time?
Degenerative disc disease progresses through predictable stages as discs age. Healthy discs contain 80% water in young adults, providing cushioning and shock absorption. Starting in the 30s, discs gradually lose water content, reducing height and flexibility. This dehydration makes discs more vulnerable to tears and bulges.
Stage 1 (Dysfunction): Minor tears develop in the outer disc layer. Patients experience intermittent pain with specific movements but maintain normal disc height on imaging. This stage responds well to activity modification and core strengthening.
Stage 2 (Instability): Disc height decreases noticeably, creating excessive motion between vertebrae. The spine becomes hypermobile at the affected level, producing frequent pain episodes. Muscles spasm to protect the unstable segment, creating chronic tension.
Stage 3 (Stabilization): Bone spurs (osteophytes) form around the disc space as the body attempts to stabilize the segment. While this natural fusion process reduces motion and pain, it also limits flexibility and can narrow nerve passages.
Risk accelerators speed degeneration:
Obesity increases mechanical load on discs by 2-3x body weight during movement
Smoking reduces blood flow to disc tissue, impairing nutrient delivery and waste removal
Occupational factors including heavy lifting, prolonged sitting, and vibration exposure
Genetics determine baseline disc quality and degeneration rate
Previous injury creates weak points that degenerate faster
Pain patterns distinguish degenerative disc disease from other causes. Patients report axial pain (centered in the spine) rather than radiating leg pain. Discomfort worsens with sitting, bending, and lifting—activities that compress discs. Pain improves with position changes, walking, and lying down. Morning stiffness lasting 30-60 minutes is common.
2026 management strategies emphasize non-opioid approaches. NSAIDs and acetaminophen control inflammation and pain. Physical therapy builds core strength to reduce disc loading. Targeted exercises strengthen multifidus muscles that stabilize individual vertebrae. Patients learn proper body mechanics for daily activities.
Advanced interventions target specific pain generators. Intradiscal injections deliver anti-inflammatory medication directly into degenerated discs. Radiofrequency ablation disables medial branch nerves transmitting pain signals from facet joints. Artificial disc replacement preserves motion in younger patients with single-level disease.
What Causes Lower Back Pain Specifically?
Lower back pain concentrates in the lumbar region (L1-L5 vertebrae) due to this area’s unique biomechanical demands. The lumbar spine supports the entire upper body’s weight while enabling forward bending, backward extension, and rotational movements. This combination of load-bearing and mobility makes the lower back vulnerable to multiple injury mechanisms.
Mechanical causes dominate:
Facet joint syndrome develops when small joints connecting vertebrae become inflamed from arthritis or injury, producing localized aching that worsens with backward bending and twisting
Sacroiliac joint dysfunction occurs where the spine meets the pelvis, creating one-sided lower back and buttock pain that mimics disc problems
Muscle imbalances between weak core muscles and tight hip flexors tilt the pelvis forward, increasing lumbar curve (hyperlordosis) and joint stress
Spinal stenosis narrows the spinal canal through bone spurs and ligament thickening, compressing nerves and causing pain with standing and walking
Injury patterns vary by activity:
Right-side lower back pain often results from asymmetrical lifting, carrying, or sports movements that overload one side
Central lower back pain typically stems from postural stress, disc problems, or arthritis affecting multiple levels
Left-side lower back pain may indicate organ issues (kidney, colon) if accompanied by fever, urinary changes, or digestive symptoms
Referred pain complicates diagnosis. Hip arthritis produces groin and buttock pain that patients interpret as lower back problems. Kidney stones create flank pain radiating to the lower back. Gynecological conditions in women can manifest as lower back discomfort.
The sedentary lifestyle epidemic drives rising lower back pain rates. Office workers who sit 8+ hours daily develop shortened hip flexors that pull the pelvis forward, weakening glutes that stabilize the pelvis, and inactive core muscles that fail to protect the spine. This muscular dysfunction creates a pain cycle that worsens without intervention.
Relief strategies address root causes:
Hip mobility exercises (90/90 stretches, pigeon pose) restore proper hip flexion and rotation
Core strengthening (planks, bird dogs, dead bugs) builds spinal stability without excessive flexion
Glute activation (bridges, clamshells, squats) rebalances hip and pelvic muscles
Movement breaks every 30-45 minutes prevent sustained postural stress
Ergonomic adjustments reduce mechanical strain during work hours
Choose inversion therapy if: you experience disc-related pain, nerve compression symptoms, or chronic lower back stiffness. Inversion tables decompress the spine by using gravity to create space between vertebrae, reducing disc pressure and nerve impingement. Start with shallow angles (20-30 degrees) for 1-2 minutes and progress gradually as tolerance builds.

How Do Lifestyle Factors Influence Back Pain?
Lifestyle choices create the foundation for back health or dysfunction. The biopsychosocial model that dominates 2026 understanding recognizes back pain as a complex interaction between physical, psychological, and social factors. This comprehensive view explains why identical structural problems produce vastly different pain experiences in different individuals.
Stress amplifies pain perception through multiple pathways. Chronic stress elevates cortisol levels, increasing systemic inflammation and pain sensitivity. Psychological tension manifests as physical muscle guarding, particularly in the neck, shoulders, and lower back. Stress also disrupts sleep quality, reducing the body’s ability to repair damaged tissues overnight.
Sleep quality directly impacts pain severity. Poor sleep lowers pain thresholds, making existing back problems feel worse. Sleep deprivation impairs tissue healing and increases inflammatory markers. Patients trapped in the pain-sleep dysfunction cycle experience progressively worsening symptoms. Prioritizing 7-9 hours of quality sleep, maintaining consistent sleep schedules, and using supportive mattresses breaks this cycle.
Nutrition provides building blocks for tissue repair and inflammation control:
Hydration maintains disc water content and cushioning ability; aim for half your body weight in ounces daily
Omega-3 fatty acids (fatty fish, flaxseed, walnuts) reduce joint inflammation and lubricate tissues
Turmeric and ginger provide natural anti-inflammatory compounds without medication side effects
Magnesium prevents muscle spasms and supports nerve function; found in leafy greens, nuts, and seeds
Vitamin D maintains bone density and muscle strength; deficiency correlates with chronic pain
Obesity multiplies mechanical stress. Each pound of excess body weight creates 4 pounds of pressure on the spine during movement. A person carrying 20 extra pounds subjects their spine to 80 additional pounds of force with each step. Weight loss of just 10% significantly reduces pain frequency and intensity in overweight individuals.
Smoking accelerates degeneration by constricting blood vessels that supply spinal discs. Reduced blood flow limits nutrient delivery and waste removal, impairing healing capacity. Smokers experience more frequent pain episodes, slower recovery from injuries, and worse surgical outcomes compared to non-smokers. Smoking cessation improves back health within months.
Physical activity paradox: Both too little and too much activity harm the back. Sedentary individuals develop weak, inflexible spines vulnerable to injury. Excessive high-impact activity without adequate recovery creates cumulative microtrauma. The optimal approach combines regular moderate activity (walking, swimming, cycling) with targeted strengthening and flexibility work.
Occupational hazards require specific countermeasures:
Manual laborers need proper lifting technique training, mechanical assists for heavy loads, and job rotation to prevent repetitive strain
Healthcare workers face high injury rates from patient handling; use transfer equipment and team lifting protocols
Truck drivers combat prolonged sitting and vibration with frequent breaks, lumbar support, and stretching routines
Office workers require ergonomic workstations, standing desk options, and movement reminders
What Are the Most Effective Relief Strategies for Back Pain?
Relief strategies in 2026 emphasize active treatment over passive approaches. Research consistently shows that movement-based therapies produce better long-term outcomes than bed rest, passive modalities, or medication alone. The most effective protocols combine multiple evidence-based interventions tailored to individual pain causes.
Physical therapy forms the cornerstone of conservative care. Licensed therapists assess movement patterns, identify muscle imbalances, and design progressive exercise programs. Treatment typically includes:
Manual therapy techniques to mobilize stiff joints and release tight muscles
Therapeutic exercises targeting specific weaknesses and movement dysfunctions
Neuromuscular re-education to correct faulty movement patterns
Modalities like heat, ice, ultrasound, or electrical stimulation for symptom management
Home exercise programs to maintain gains between sessions
Core strengthening protects the spine more effectively than any other intervention. However, 2026 protocols avoid traditional crunches and sit-ups that increase disc pressure. Instead, spine surgeon Dr. Collin Haines recommends exercises that maintain neutral spine position:
Planks (front, side, and variations) build endurance in stabilizing muscles
Bird dogs coordinate opposite arm and leg movements while maintaining spinal stability
Dead bugs challenge core control while lying supine
Pallof presses resist rotational forces that stress the spine
Carries (farmer’s walk, suitcase carry) build functional core strength during movement
Inversion therapy provides drug-free decompression by using gravity to separate vertebrae and reduce disc pressure. Clinical studies demonstrate that inversion reduces back pain and improves function in patients with disc problems, sciatica, and chronic lower back pain. Benefits include:
Reduced pressure on compressed discs and nerves
Increased space between vertebrae
Improved spinal alignment
Enhanced circulation to spinal tissues
Relaxation of tense back muscles
Start conservatively with 20-30 degree angles for 1-2 minutes once or twice daily. Progress gradually to steeper angles and longer durations as tolerance builds. Contraindications include uncontrolled high blood pressure, glaucoma, recent stroke, and pregnancy. Consult healthcare providers before starting inversion therapy if you have any medical conditions.
Anti-inflammatory strategies reduce pain triggers:
Ice therapy (first 48-72 hours after injury) constricts blood vessels and reduces swelling
Heat therapy (after acute phase) increases blood flow and relaxes muscles
NSAIDs (ibuprofen, naproxen) control inflammation when used short-term
Topical analgesics provide localized relief without systemic side effects
Dietary modifications emphasizing anti-inflammatory foods
Movement remains essential even during pain episodes. Complete bed rest beyond 1-2 days worsens outcomes by causing muscle atrophy, joint stiffness, and psychological deconditioning. Instead, maintain activity within pain tolerance, gradually increasing duration and intensity as symptoms improve.
2026 technology innovations enhance traditional approaches:
Smart posture wearables provide haptic feedback when users slouch, training better alignment habits
FDA-cleared VR therapy uses immersive environments to distract from pain and break fear-avoidance patterns
Telehealth physical therapy expands access to expert guidance through video consultations and app-based exercise programs
Wearable TENS units deliver electrical stimulation for pain relief during daily activities
Injection therapies target specific pain generators when conservative care plateaus:
Epidural steroid injections deliver anti-inflammatory medication to compressed nerve roots
Facet joint injections reduce arthritis pain in spinal joints
Trigger point injections release persistent muscle knots
Platelet-rich plasma (PRP) uses concentrated growth factors to promote healing in damaged tissues
Minimally invasive procedures offer alternatives to traditional surgery:
Radiofrequency ablation disables pain-transmitting nerves for 6-12 months of relief
Spinal cord stimulation uses electrical signals to interrupt pain messages
Interspinous spacers create space between vertebrae in stenosis patients
Minimally invasive lumbar decompression removes tissue compressing nerves through small incisions
Surgery remains the last resort for specific indications: progressive neurological deficits (weakness, numbness), cauda equina syndrome (loss of bowel/bladder control), or failure of 6-12 months of comprehensive conservative care. Modern surgical techniques emphasize tissue preservation and faster recovery compared to traditional open procedures.
When Should You Seek Professional Medical Care for Back Pain?
Most back pain episodes resolve within 4-6 weeks with self-care measures. However, certain warning signs indicate serious underlying conditions requiring immediate medical evaluation. Understanding these red flags prevents delays in treating potentially dangerous problems.
Seek emergency care immediately for:
Cauda equina syndrome symptoms: loss of bowel or bladder control, saddle anesthesia (numbness in groin/inner thighs), progressive leg weakness
Severe trauma: back pain following significant falls, motor vehicle accidents, or direct impacts
Fever with back pain: suggests possible spinal infection (discitis, osteomyelitis)
Unexplained weight loss: combined with back pain may indicate malignancy
History of cancer: new back pain in cancer patients requires evaluation for metastatic disease
Schedule prompt medical evaluation (within days) for:
Pain persisting beyond 4-6 weeks despite self-care
Progressive neurological symptoms (increasing numbness, weakness, or tingling)
Pain that worsens at night or at rest (suggests non-mechanical causes)
Pain radiating below the knee (indicates possible nerve root compression)
Severe pain unrelieved by position changes or over-the-counter medications
Age over 50 with new-onset back pain (higher risk of serious pathology)
History of osteoporosis (increased fracture risk)
Diagnostic imaging helps identify structural problems when indicated. X-rays reveal bone abnormalities, alignment issues, and arthritis. MRI scans visualize soft tissues including discs, nerves, and ligaments. CT scans provide detailed bone images when MRI is contraindicated. However, imaging should follow clinical evaluation rather than replace it—many imaging findings don’t correlate with symptoms.
The diagnostic process typically includes:
Medical history: onset, location, quality, radiation, aggravating/relieving factors, previous episodes
Physical examination: posture assessment, range of motion testing, neurological evaluation, palpation for tenderness
Special tests: straight leg raise, slump test, reflexes, sensation mapping, strength testing
Imaging studies: ordered based on clinical findings and red flags
Diagnosis: identifying specific pain generators and contributing factors
Treatment plan: evidence-based interventions matched to diagnosis
Specialist referrals address complex cases:
Physiatrists (physical medicine and rehabilitation doctors) coordinate non-surgical care
Pain management specialists provide advanced injection therapies and interventional procedures
Neurosurgeons or orthopedic spine surgeons evaluate surgical candidates
Rheumatologists manage inflammatory arthritis affecting the spine
Physical therapists design and supervise exercise-based rehabilitation
Avoid common mistakes: Doctor shopping for opioid prescriptions, demanding imaging without clinical indication, expecting passive treatments to cure active problems, and delaying evidence-based care while pursuing unproven alternative therapies.
How Can You Prevent Future Back Pain Episodes?
Prevention strategies protect against initial injury and reduce recurrence risk in those with previous episodes. Since 80% of people experience back pain at some point, and 50% of those with one episode develop recurrent problems, prevention deserves priority attention.
Movement quality trumps quantity. Proper body mechanics during daily activities prevent cumulative microtrauma:
Lifting technique: Bend knees, keep load close to body, avoid twisting while carrying weight, engage core before lifting
Pushing vs. pulling: Push heavy objects when possible (uses stronger leg muscles), keep elbows bent when pulling
Reaching overhead: Use step stools instead of overreaching, avoid prolonged overhead work
Getting in/out of cars: Sit first, then swing legs in together; reverse when exiting
Workspace ergonomics reduce postural stress during desk work:
Monitor position: Top of screen at or slightly below eye level, arm’s length distance
Chair setup: Lumbar support maintains natural curve, feet flat on floor or footrest, thighs parallel to ground
Keyboard/mouse: Elbows at 90 degrees, wrists neutral (not bent up or down)
Phone use: Headset or speakerphone prevents neck strain from cradling phone
Standing desk: Alternate sitting and standing every 30-60 minutes
Regular exercise builds resilience against injury. The most protective programs combine:
Cardiovascular activity: 150 minutes weekly of moderate-intensity exercise (walking, swimming, cycling)
Strength training: 2-3 sessions weekly targeting major muscle groups, emphasizing core and lower body
Flexibility work: Daily stretching for hip flexors, hamstrings, and thoracic spine
Balance training: Single-leg exercises and stability work prevent falls and improve body control
Pre-activity preparation reduces injury risk:
Warm-up: 5-10 minutes of light activity increases tissue temperature and blood flow
Dynamic stretching: Movement-based stretches prepare muscles for activity demands
Progressive loading: Gradually increase weight, distance, or intensity rather than sudden jumps
Recovery time: Allow 48 hours between intense sessions for tissue repair
Maintain healthy body weight to reduce mechanical stress. Even modest weight loss (5-10% of body weight) significantly decreases pain frequency in overweight individuals. Combine calorie reduction with increased activity for sustainable results.
Manage stress effectively to prevent muscle tension and pain amplification:
Mindfulness meditation: 10-20 minutes daily reduces stress hormones and pain perception
Deep breathing: Diaphragmatic breathing activates relaxation response
Progressive muscle relaxation: Systematic tension and release of muscle groups
Regular breaks: Step away from stressors throughout the day
Sleep optimization supports tissue healing and pain control:
Mattress selection: Medium-firm mattresses suit most back pain patients; replace every 7-10 years
Sleep position: Side sleeping with pillow between knees maintains spinal alignment; back sleeping with pillow under knees reduces lumbar stress
Pillow support: Neck pillow maintains cervical curve without excessive flexion or extension
Sleep hygiene: Consistent schedule, cool dark room, limit screens before bed
Regular maintenance care catches problems early:
Annual check-ups: Screen for risk factors and address minor issues before they worsen
Periodic physical therapy: “Tune-up” sessions every 3-6 months for those with recurrent problems
Ongoing exercise: Maintain strength and flexibility gains rather than stopping after pain resolves
Body awareness: Notice and address minor aches before they escalate
Frequently Asked Questions About Causes of Back Pain
What is the number one cause of back pain?
Muscle strain or sprain causes the majority of back pain cases. This injury results from overuse, improper lifting technique, sudden movements, or repetitive stress that tears muscle fibers or ligaments. Most muscle-related back pain resolves within 2-6 weeks with rest, ice/heat therapy, gentle movement, and over-the-counter pain relievers.
Can back pain be caused by stress alone?
Yes, psychological stress directly triggers back pain through muscle tension and increased pain sensitivity. Chronic stress elevates cortisol levels, amplifying inflammation and lowering pain thresholds. Stress also causes unconscious muscle guarding, particularly in the neck, shoulders, and lower back. Managing stress through relaxation techniques, exercise, and adequate sleep reduces stress-related back pain.
Why does my lower back hurt when I sit?
Sitting increases disc pressure by 40% compared to standing and often involves forward-leaning posture that stresses spinal structures. Prolonged sitting also tightens hip flexors and weakens core muscles, creating imbalances that strain the lower back. Take movement breaks every 30-45 minutes, use proper ergonomic setup, and strengthen core muscles to reduce sitting-related pain.
How do I know if my back pain is serious?
Seek immediate medical care for back pain accompanied by loss of bowel or bladder control, progressive leg weakness, numbness in the groin area, fever, or unexplained weight loss. Schedule prompt evaluation for pain lasting beyond 6 weeks, pain radiating below the knee, nighttime pain that wakes you, or pain following significant trauma. Most other back pain responds to conservative self-care measures.
Does inversion therapy really work for back pain?
Clinical research demonstrates that inversion therapy reduces back pain and improves function in patients with disc problems, sciatica, and chronic lower back pain. Inversion uses gravity to decompress the spine, reducing pressure on discs and nerves while improving spinal alignment. Start with shallow angles (20-30 degrees) for 1-2 minutes and progress gradually. Avoid inversion if you have uncontrolled high blood pressure, glaucoma, or recent stroke.
What sleeping position is best for back pain?
Side sleeping with a pillow between your knees maintains spinal alignment and reduces stress on the lower back. Back sleeping with a pillow under your knees also works well by maintaining the spine’s natural curves. Avoid stomach sleeping, which forces neck rotation and increases lumbar extension. Use a supportive mattress (medium-firm for most people) and replace pillows every 1-2 years.
Can poor posture cause permanent back damage?
Poor posture creates sustained mechanical stress that accelerates disc degeneration and joint wear over years or decades. While posture alone rarely causes acute injury, chronic postural dysfunction leads to muscle imbalances, joint stiffness, and increased injury risk. The good news: correcting posture through ergonomic adjustments, stretching, and strengthening exercises reverses many negative effects before permanent damage occurs.
How long does it take for back pain to heal?
Acute muscle strain typically improves within 2-6 weeks with appropriate self-care. Disc-related pain often resolves within 6-12 weeks as the body resorbs herniated material. Chronic pain from degenerative conditions requires ongoing management rather than complete healing. Factors affecting healing time include injury severity, age, overall health, treatment compliance, and whether you continue activities that aggravate the problem.
What exercises should I avoid with back pain?
Avoid exercises that increase disc pressure or stress injured tissues: traditional sit-ups and crunches, toe touches with straight legs, heavy deadlifts or squats during acute pain, high-impact activities like running on hard surfaces, and exercises that cause sharp pain or radiating symptoms. Focus instead on core stabilization exercises, gentle stretching, and low-impact cardiovascular activities like walking or swimming.
Can back pain be a sign of something more serious?
While most back pain stems from mechanical problems (muscle strain, disc issues, arthritis), serious underlying conditions occasionally cause back pain. Red flags include cancer history, unexplained weight loss, fever, nighttime pain, age over 50 with new-onset pain, recent infection, intravenous drug use, or prolonged steroid use. These factors increase risk for spinal infection, tumor, or fracture requiring immediate evaluation.
Does losing weight help back pain?
Yes, weight loss significantly reduces back pain in overweight individuals. Each pound of excess body weight creates approximately 4 pounds of pressure on the spine during movement. Losing just 10% of body weight decreases mechanical stress, reduces inflammatory markers, and improves mobility. Combine calorie reduction with regular exercise for sustainable weight loss and maximum back pain relief.
What’s the difference between acute and chronic back pain?
Acute back pain lasts less than 6 weeks and typically results from specific injury or strain. It responds well to conservative treatment and usually resolves completely. Chronic back pain persists beyond 12 weeks and often involves multiple contributing factors including structural problems, muscle imbalances, and central nervous system sensitization. Chronic pain requires comprehensive management addressing physical, psychological, and lifestyle factors rather than expecting complete cure.
Conclusion
The causes of back pain span a spectrum from simple muscle strain to complex degenerative conditions, but most cases respond favorably to evidence-based conservative treatment. Understanding your specific pain triggers—whether mechanical stress from poor posture, disc problems compressing nerves, arthritis degrading joints, or lifestyle factors amplifying symptoms—empowers you to pursue targeted relief strategies.
The 2026 approach to back pain emphasizes active treatment over passive interventions. Core strengthening, movement quality, and lifestyle modifications provide more lasting relief than medication or passive therapies alone. Inversion therapy offers a drug-free option for spinal decompression that complements other conservative treatments. When conservative care plateaus, minimally invasive procedures target specific pain generators without the risks of traditional surgery.
Take action today:
Assess your risk factors: Identify modifiable contributors like poor posture, sedentary habits, excess weight, or stress
Start moving: Begin gentle activity within pain tolerance rather than waiting for complete pain resolution
Build core strength: Focus on stabilization exercises that protect your spine during daily activities
Optimize your environment: Adjust workspace ergonomics and sleep setup to reduce mechanical stress
Consider inversion therapy: Explore spinal decompression as a non-surgical relief option if you have disc-related pain
Seek professional guidance: Consult healthcare providers for persistent pain, neurological symptoms, or red flag warnings
Back pain affects millions, but it doesn’t have to control your life. Armed with knowledge about causes and evidence-based relief strategies, you can take meaningful steps toward lasting improvement and prevention of future episodes.
SEO Meta Title
Causes of Back Pain: Relief Strategies & Prevention Tips
Meta Description
Discover common causes of back pain from muscle strain to disc problems, plus proven relief strategies including inversion therapy, exercises, and lifestyle changes.
Tags
causes of back pain, lower back pain, herniated disc, muscle strain, degenerative disc disease, inversion therapy, back pain relief, spinal decompression, core strengthening, posture correction, sciatica, chronic back pain