Approximately 21% of patients using inversion therapy required surgery within two years, compared to 43% at four years in matched control groups—a striking difference that demands explanation. The science behind spinal decompression through inversion tables centers on gravity-assisted traction that temporarily increases disc space and reduces mechanical compression on nerve roots. Understanding the biomechanics reveals why this simple intervention produces measurable relief for many patients with lumbar disc disease and sciatica.
Think of your spine like a stack of cushions compressed by a heavy weight. Inversion therapy flips that weight, allowing the cushions to expand and relieve pressure on anything trapped between them.
Key Takeaways
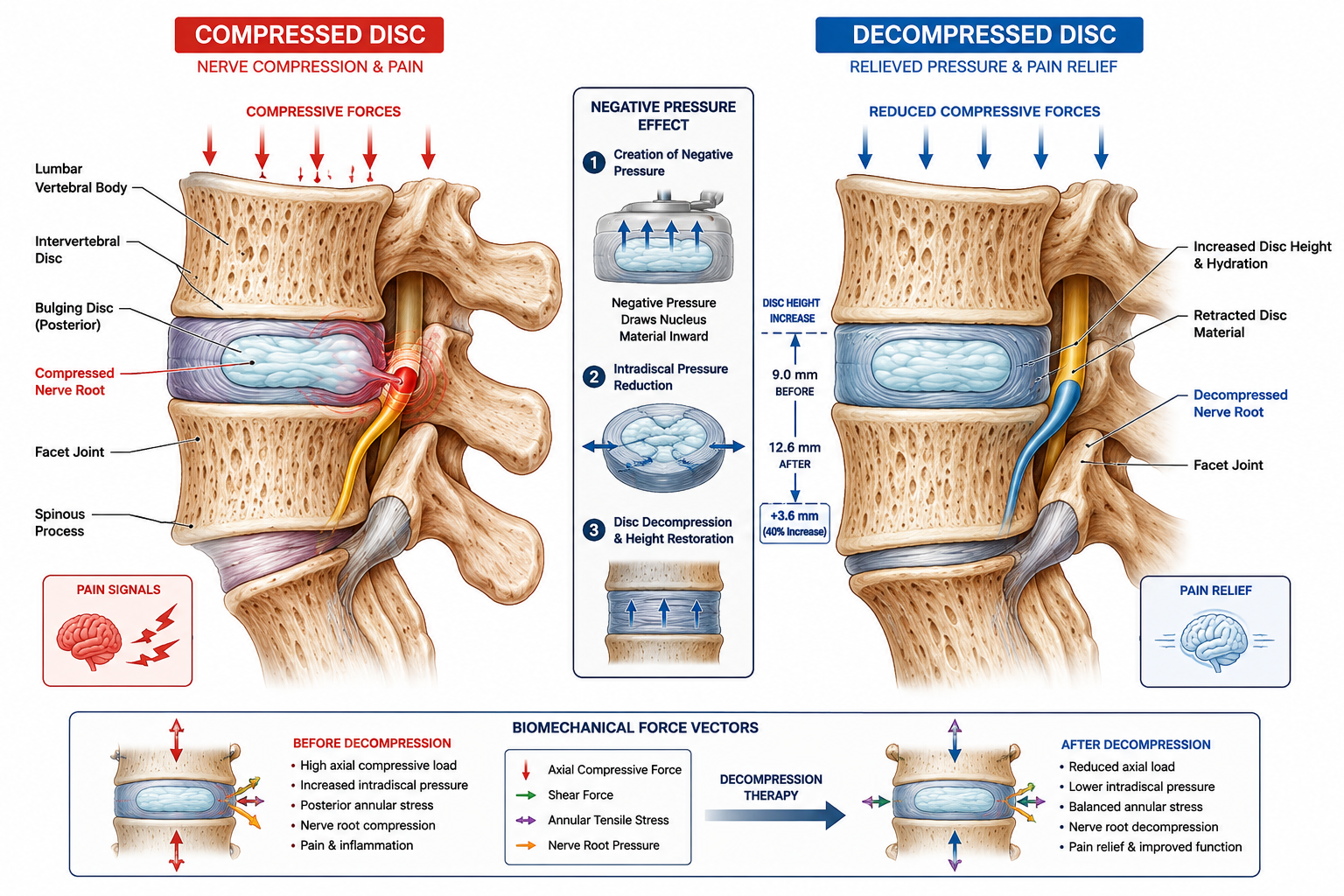
- Gravity-assisted traction creates negative intradiscal pressure that may draw bulging disc material away from nerve roots
- Clinical evidence shows inversion therapy reduced surgery rates from 43% to 21% in selected lumbar disc patients
- Temporary relief occurs through biomechanical distraction of vertebrae, not permanent structural correction
- Safety considerations remain critical—inversion increases cranial pressure and poses risks for cardiovascular and eye conditions
- Professional decompression offers more controlled, segment-specific traction than home inversion tables
How Gravity-Assisted Traction Creates Negative Intradiscal Pressure
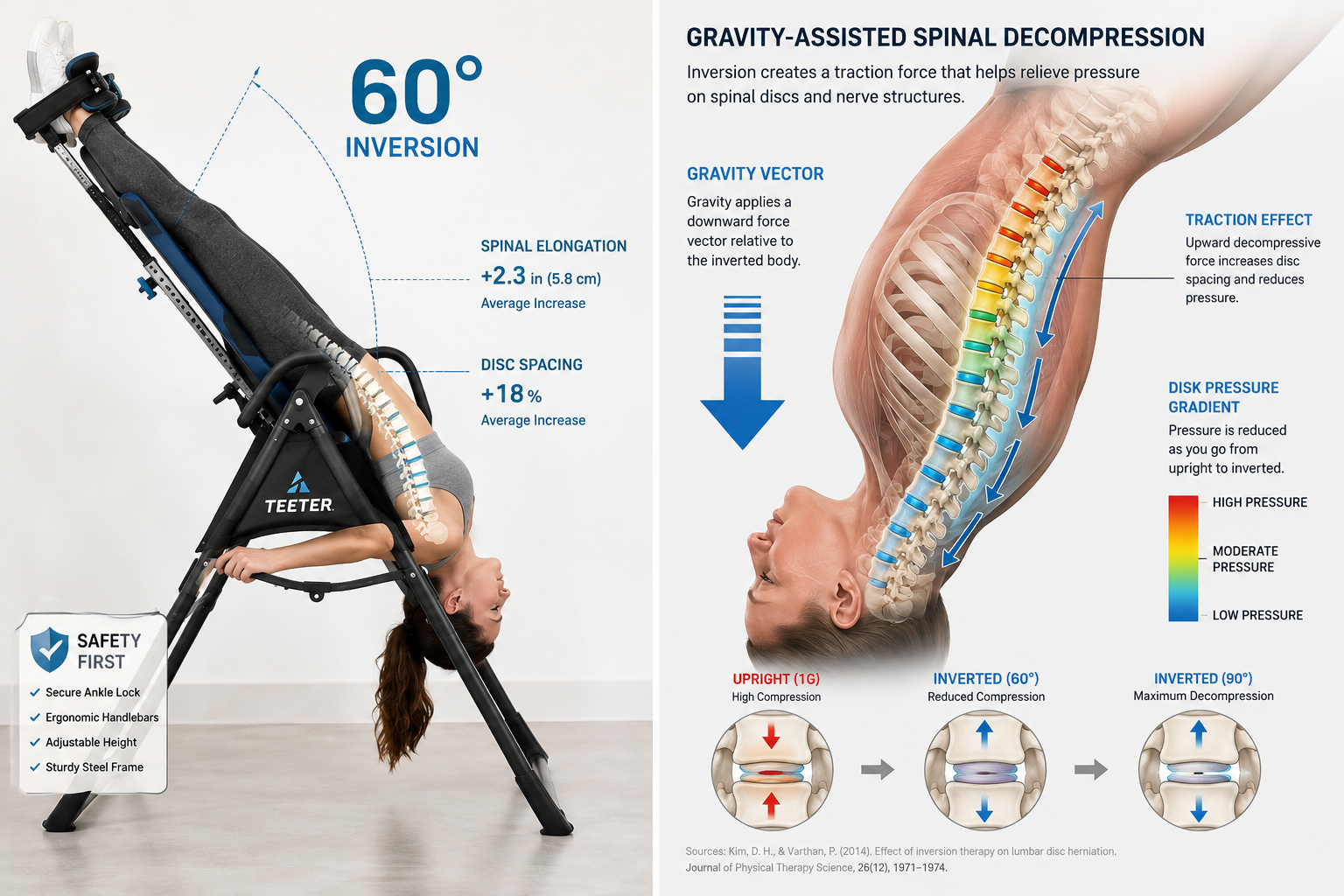
The biomechanics of spinal decompression through inversion tables operate on a straightforward principle: gravity reverses its usual compressive force on the spine. When you invert your body, gravity pulls your torso away from your pelvis, creating axial traction along the lumbar spine. This traction generates negative pressure within the intervertebral discs—the cushioning structures between vertebrae.
Research demonstrates that this negative pressure serves a therapeutic purpose. The pressure gradient may help draw herniated or bulging disc material back toward the center of the disc, reducing mechanical compression on adjacent nerve roots. Nerve roots exit the spinal canal through small openings called foramina, and when disc material protrudes into these spaces, it creates the radiating pain characteristic of sciatica and radiculopathy.
The Mechanical Forces at Work
During inversion, several biomechanical changes occur simultaneously:
- Vertebral separation increases by 1-3 millimeters at affected segments
- Foraminal space expands, reducing nerve root impingement
- Paraspinal muscles stretch and relax, decreasing protective muscle spasm
- Intradiscal pressure drops below baseline resting levels
The forces that gravity exerts during inversion directly counteract the compressive loads your spine experiences during upright activities. Standing, sitting, and lifting all compress your discs and narrow the spaces where nerves exit. Inversion temporarily reverses this compression, providing a mechanical unloading of stressed spinal structures.
For patients with herniated discs compressing nerves, this temporary decompression can produce immediate symptom relief. The reduction in nerve-root irritation translates to decreased pain signals traveling to the brain.
The Evidence: What Clinical Studies Actually Show
The strongest peer-reviewed evidence for inversion therapy comes from a Newcastle University study that tracked patients with lumbar disc disease over multiple years. The results revealed substantial differences in surgical intervention rates between groups using inversion therapy and matched controls.
Specifically, the inversion therapy group showed:
- 21% surgery rate at 2 years versus 39% in controls
- Continued benefit with only 21% requiring surgery even at longer follow-up
- Symptom improvement measured by validated pain and disability scales
An earlier randomized controlled trial demonstrated even more dramatic results: inversion therapy reduced the need for surgery in three out of four patients who had been placed on a waiting list for discectomy procedures. These patients were already scheduled for surgical intervention, yet inversion therapy provided sufficient relief that surgery became unnecessary.
Understanding the Limitations
Despite these encouraging findings, major medical institutions maintain a cautious stance. Cleveland Clinic explicitly states that research remains “mixed and generally low-quality” with limited evidence supporting broad claims about inversion tables. The studies showing benefit are relatively small-scale and lack the multi-center, large-population design that would establish inversion as a standard treatment.
The current evidence suggests inversion tables provide:
✅ Temporary symptom relief for selected patients with disc-related nerve compression
✅ Reduced surgery rates in some clinical populations
✅ Short-term improvements in pain and disability scores
❌ Not a definitive cure for structural disc disease
❌ Not appropriate for all back pain conditions
❌ Not universally effective across all patient populations
For comprehensive guidance on selecting appropriate equipment, consult our complete inversion table buying guide.
Inversion Tables vs. Professional Spinal Decompression: Key Differences
A critical distinction exists between home inversion tables and clinical spinal decompression machines. Both aim to relieve nerve-root pressure, but they accomplish this goal through different mechanisms and levels of control.
Inversion Tables: Gravity-Based Traction
Inversion tables use your body weight and gravity to create traction. The amount of decompressive force depends on:
- Inversion angle (partial inversion at 20-30° versus full inversion at 60-90°)
- Body weight distribution
- Duration of inversion session
- User positioning and relaxation
This approach offers simplicity and accessibility for home use but provides less precise control over which spinal segments receive traction. The decompressive force distributes across the entire lumbar and thoracic spine rather than targeting specific problem areas.
Professional Decompression: Controlled, Segment-Specific Traction
Clinical spinal decompression machines employ computer-controlled, motorized systems that deliver precise traction to targeted spinal segments. These devices:
- Gradually increase traction force to avoid muscle guarding
- Cycle between traction and relaxation phases
- Target specific vertebral levels identified through imaging
- Monitor patient response in real-time
Physical therapists and chiropractors adjust treatment parameters based on individual patient anatomy and response. This supervised, customized approach aims for longer-term structural improvements rather than temporary symptom relief.
For patients considering alternatives, our comparison of inversion tables versus chiropractic care provides additional perspective on treatment options.
Safety Considerations: Who Should Avoid Inversion Therapy
The science behind spinal decompression through inversion tables includes important physiological effects beyond the spine. Inversion increases blood flow to the head and raises intracranial pressure—a serious concern for specific patient populations.
High-Risk Conditions
Medical authorities identify several conditions that contraindicate inversion therapy:
| Condition | Risk |
|---|---|
| Hypertension | Sudden blood pressure spikes |
| Glaucoma | Increased intraocular pressure |
| Heart disease | Cardiovascular stress |
| Stroke history | Risk of recurrent cerebrovascular events |
| Retinal detachment | Worsening of eye condition |
| Pregnancy | Fetal positioning concerns |
Patients with these conditions should consult healthcare providers before attempting inversion therapy. Our detailed safety guide for hypertension patients addresses cardiovascular concerns specifically.
Safe Usage Protocols
For appropriate candidates, safe inversion therapy follows these principles:
- Start gradually with 1-2 minutes at shallow angles (20-30°)
- Progress slowly over weeks as tolerance builds
- Never invert immediately after eating
- Use safety straps and proper ankle supports
- Have assistance available during initial sessions
Understanding common myths about inversion tables helps patients separate evidence-based benefits from marketing hype.
The Physiological Mechanism: Why Temporary Relief Occurs
The science behind spinal decompression reveals why inversion therapy produces temporary rather than permanent changes. The biomechanical effects reverse when you return to an upright position and gravity resumes its compressive force.
Immediate Effects During Inversion
While inverted, your spine experiences:
- Axial distraction that increases disc height
- Reduced nerve-root compression from expanded foraminal space
- Muscle relaxation as paraspinal muscles stretch
- Decreased pain signals from decompressed neural structures
These changes occur within minutes and provide immediate symptom relief for many users. The negative intradiscal pressure created during inversion may temporarily reduce disc bulge size, though imaging studies show this effect reverses after returning upright.
Post-Inversion Benefits
After completing an inversion session, several effects may persist:
- Reduced muscle spasm from the stretching effect
- Improved circulation to spinal tissues
- Decreased inflammation around irritated nerve roots
- Enhanced mobility from reduced pain and stiffness
Regular inversion therapy may provide cumulative benefits through repeated decompression cycles, though the evidence for long-term structural changes remains limited. Patients who combine inversion with other therapies—including nutrition strategies that support spinal health—may experience enhanced outcomes.
Why Permanent Changes Don’t Occur
Inversion tables do not permanently reposition herniated disc material or reverse degenerative disc disease. The biomechanical forces during inversion are insufficient to create lasting structural changes in disc architecture. Once you return upright, gravitational compression resumes and disc spaces return to baseline dimensions.
This explains why inversion therapy works best as an ongoing management strategy rather than a one-time cure. Patients who experience benefit typically need regular sessions to maintain symptom relief.
Practical Application: Maximizing Therapeutic Benefit
Understanding the science behind spinal decompression helps patients optimize their inversion therapy approach. Evidence-based protocols maximize benefit while minimizing risk.
Optimal Session Parameters
Research and clinical experience suggest these guidelines:
- Frequency: 2-3 sessions daily for acute symptoms; 1 session daily for maintenance
- Duration: 3-5 minutes per session initially, progressing to 10-15 minutes
- Angle: Start at 20-30° and gradually increase to 60° as tolerated
- Timing: Avoid inversion within 2 hours of meals
Complementary Strategies
Inversion therapy produces better results when combined with:
- Core strengthening exercises to support spinal stability
- Flexibility training to maintain range of motion
- Proper ergonomics during daily activities
- Weight management to reduce spinal loading
Patients with scoliosis or spinal alignment issues should consult specialists before beginning inversion therapy, as asymmetric spinal conditions may require modified protocols.
Monitoring Response
Track your response to inversion therapy by noting:
- Pain intensity before and after sessions
- Functional improvements in daily activities
- Medication usage changes
- Sleep quality modifications
If symptoms worsen or new problems develop, discontinue inversion and consult a healthcare provider. Some patients experience increased lower back pain from improper technique or inappropriate use.
Current Expert Consensus and Future Directions
The science behind spinal decompression through inversion tables continues to evolve as researchers conduct higher-quality studies. Current expert consensus acknowledges both the potential benefits and significant limitations of this approach.
What Experts Agree On
Medical professionals generally concur that:
- Selected patients with disc-related nerve compression may benefit from inversion therapy
- Temporary symptom relief represents a realistic expectation
- Safety screening remains essential before beginning inversion
- Professional decompression offers more controlled treatment for serious conditions
- Inversion tables serve best as adjunctive therapy rather than primary treatment
No major medical society has endorsed inversion tables as a standard treatment for radiculopathy or nerve-root compression. The evidence base, while promising, lacks the scale and quality needed for broad clinical recommendations.
Research Gaps
Future studies should address:
- Optimal treatment protocols for different spinal conditions
- Long-term outcomes beyond 2-4 years
- Comparative effectiveness versus other conservative treatments
- Predictors of response to identify ideal candidates
- Mechanisms of benefit through advanced imaging studies
Until higher-quality evidence emerges, inversion therapy remains a patient-selected option that may provide meaningful relief for some individuals with nerve-root compression from disc disease.
Conclusion
The science behind spinal decompression through inversion tables rests on solid biomechanical principles: gravity-assisted traction creates negative intradiscal pressure that temporarily reduces nerve-root compression. Clinical evidence demonstrates that selected patients with lumbar disc disease experience symptom improvement and reduced surgery rates with regular inversion therapy. However, this intervention provides temporary relief rather than permanent structural correction, and significant safety considerations limit its appropriateness for many patients.
Take these action steps to apply this knowledge:
- Consult your healthcare provider to determine if inversion therapy suits your specific spinal condition
- Screen for contraindications, especially cardiovascular, blood pressure, and eye conditions
- Start conservatively with short sessions at shallow angles, progressing gradually
- Combine inversion with complementary strategies like core strengthening and proper ergonomics
- Monitor your response objectively and adjust your approach based on results
For patients who are appropriate candidates, inversion tables offer an accessible, home-based option for managing nerve-root compression symptoms. Understanding the underlying biomechanics helps set realistic expectations and optimize therapeutic benefit. While not a cure for structural disc disease, gravity-assisted spinal decompression provides a valuable tool in the comprehensive management of certain back pain conditions.
Review our guide to avoiding common dangers before beginning inversion therapy to ensure safe, effective use.
SEO Meta Title: Spinal Decompression Science: How Inversion Tables Work